The Vitals
Over 1 million Americans died from suicide or drug or alcohol related deaths from 2006-15. The U.S. boasts more opioids per capita than any other country in the world. These “deaths of despair” are most prevalent in the American heartland, in places where manufacturing and other blue-collar jobs have disappeared. Policy for opioid and related addictions, at least at the federal level, has focused on saving addicts from overdose death by extending the supply of “opioid antagonist” medications to first responders and relevant medical personnel. What has been missing is an approach that addresses the epidemic’s root causes by dealing with both demand and supply.
-
The U.S. is the only wealthy country in the world where life expectancy has been declining rather than going up for the past three years, due to preventable deaths among less than college-educated whites.
-
Over 1 million Americans died from suicide or drug or alcohol related deaths from 2006-15.
-
The crisis is both demand and supply driven: desperation related to the decline in the quantity and quality of low-skilled jobs collided with a market flooded with opioids and other drugs.
A Closer Look
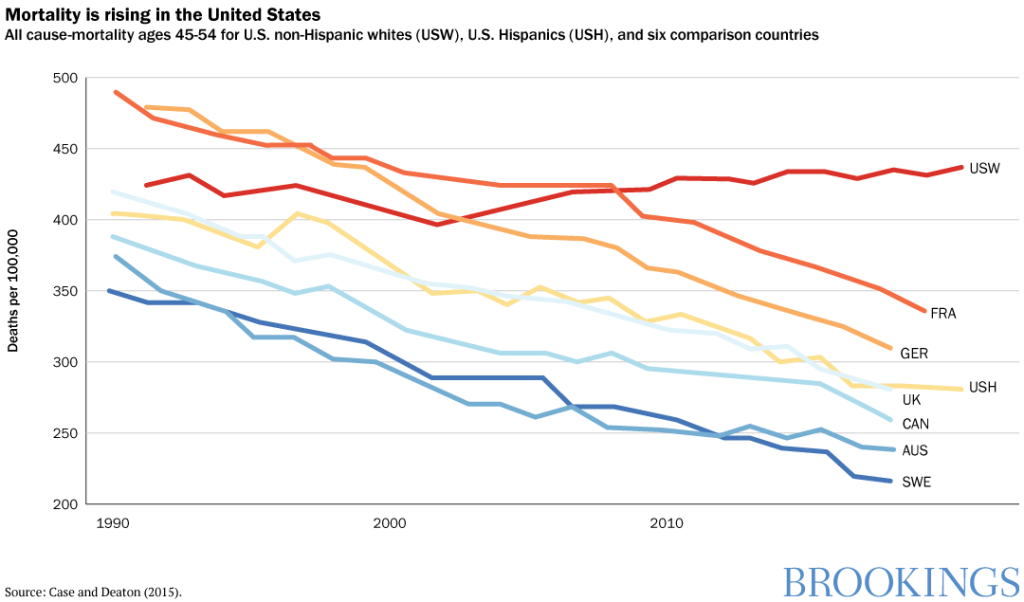
As the only wealthy country in the world where mortality rates are climbing, the United States is in the midst of a social crisis (some new data for Scotland suggests similar patterns, although not on the same scale) . The trend is primarily driven by preventable “deaths of despair”—suicides, drug overdose, and alcohol related deaths—among less than college-educated whites in their middle-aged years. In contrast, blacks and Hispanics, who have lower levels of life expectancy and objectively face greater disadvantages, have been making gradual progress and remain significantly more optimistic than whites .
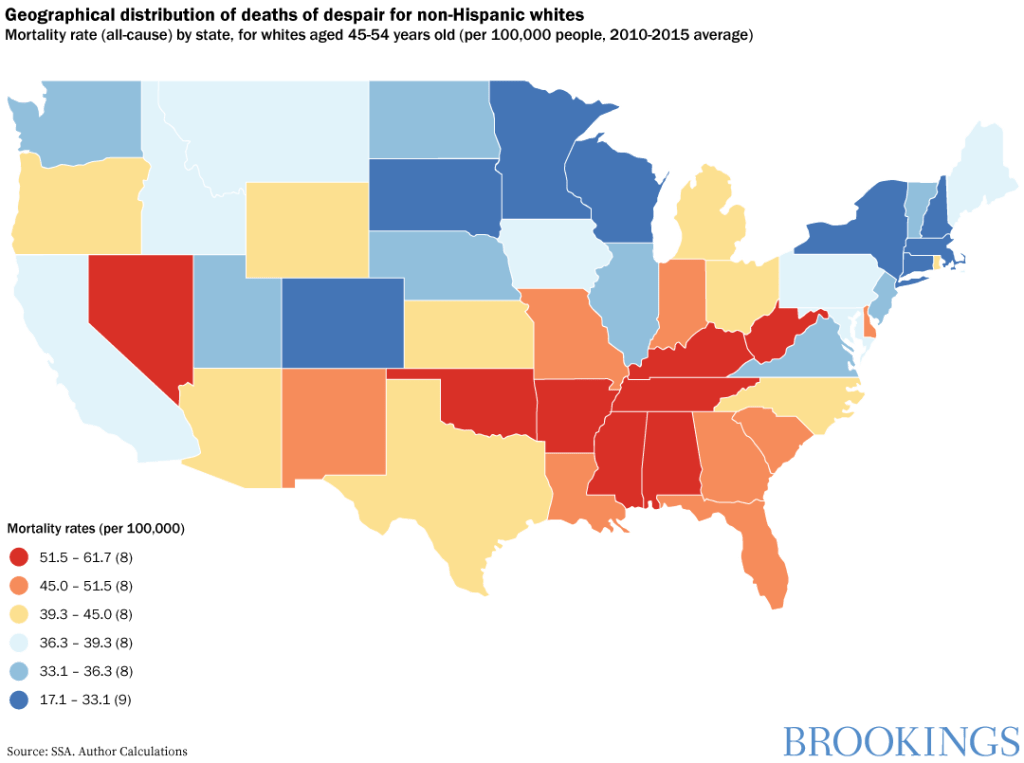
Deaths of despair are most prevalent in the American
heartland, in places where manufacturing and other blue-collar jobs have
disappeared, and where the communities that formerly supported these industries
are experiencing high associated social costs. The loss of purposeful
employment—and
hope more generally—is
an important part of the explanation of trends in both addiction and mortality.
Sergio
Pinto and I find that the same cohorts who are most likely to suffer
from premature mortality—less
than college-educated whites in rural or suburban parts of the country—have much higher levels of reported
ill-being, with little hope for the future and high levels of worry.
How bad is the crisis?
The numbers are daunting. Over 1 million Americans died
from suicide or drug or alcohol related deaths from 2006-15, with 127,500 in
2015 alone. According to the Centers for Disease Control and Prevention’s
latest data, overdose deaths finally tapered in 2018, but there were still 68,000
deaths. The U.S. still boasts more opioids per capita than
any other country in the world, and more people report to have
experienced pain the previous day than respondents in 30 other countries around
the world, many of them less wealthy than we are.
There were some modest changes in demographic and locational patterns in
2018, with the trends in most heartland states holding steady and even declining
in some instances. At the same time, overdoses continued to rise in some
mid-Atlantic states and began to increase in many Western ones for the first
time. Western
cities saw a new pattern in overdose deaths among older urban black men—many of them former
crack or heroin addicts who acquired access to the particularly lethal
drug Fentanyl in recent years.
What are the root causes?
The term “deaths of despair,” meanwhile, suggests an economic or social
crisis rather than a health one. It is all three, and it is both demand and
supply driven. Since the 1970s, the decline in manufacturing has hit particular
regions and communities much more than others. As Justin Pierce and Peter Schott
show, the mortality crisis hit places with industries where Chinese competition
increased most intensely. More generally, it reflects an increasing trend of
automation replacing low-skill jobs. The same communities that saw pronounced
declines in employment also experienced decreases in marriage rates, increases
in the percentage
of prime-aged males out of the labor force, higher rates of reported pain, and
higher opioid prescription rates. The latter two trends relate in
part to the toll that manufacturing and mining jobs take on workers’ health.
Higher levels of reported pain and related opioid use are also due to strategic
supply strategies, first by the pharmaceutical industry and subsequently by
drug traffickers. The outcome was literally a perfect storm.
What can policymakers do?
Policy for
opioid and related addictions, at least at the federal level, has focused on
saving addicts from overdose death by extending the supply of “opioid
antagonist” medications such as Naloxone
to first responders and relevant medical personnel. While more comprehensive efforts
to prevent suicide—such as the work done by the Substance Abuse and Mental
Health Services Administration—have existed for years, they have
not received much support from the current U.S. administration. Meanwhile, the
current efforts—$3.3 billion in grants to states
since 2017 for prevention, treatment, and recovery services—are
slated to lose funding next year.
What is missing is an approach that addresses the epidemic’s root causes by dealing with both demand and supply issues. While the oversupply of opioids has become an issue in the courts—such as the case in New York against the Sackler family and Purdue Pharma—the Trump administration has not attempted to deal with the more fundamental problem. The recent lawsuit against Johnson & Johnson, for example, was again at the state level (Oklahoma), and it is unclear how much of the settlement gains will actually reach the victims versus going to pay legal fees. There is still debate about how much victims will benefit from the multi-state Purdue Pharma suit as it settles. Meanwhile, while there has been more medical scrutiny in recent years on the prescription of opioids, variance across places remains tremendous.
There is still no comprehensive policy approach for addressing the more complex demand problem. Addressing a crisis of desperation defies most standard policy definitions and policy prescriptions. Understanding differential resilience across population cohorts is even further from current policy discussions. Yet the root causes of the problem—which stem from the decline of the working class, the erosion of families, communities, and social capital, and an inadequate public health care system—are not going away and, even worse, are likely to spill over into the next generation. Many of those who are either addicted or have died from deaths of despair, for example, have children who are displaying signs of stress from experiences ranging from general neglect to witnessing their parents’ overdoses. Such experiences will have a long reach into their adulthood.
Which interventions have been successful?
How to
restore hope? How to teach resilience? This is not an easy task, but there are
lessons, most of which come from local level efforts.
Desperation
can be reversed, as recent research shows.
Interventions and simple programs that help people have better outlooks include
increasing access to volunteering, the arts, and shared green spaces, all of
which increase sense of purpose and reduce isolation. Interacting with
community members raises the well-being of people who have retired or dropped
out of the labor force and are otherwise at home alone and vulnerable to
depression and despair.
In 2015, researchers and the City of Santa Monica designed a well-being tracking index and related interventions in that community. When the survey identified social isolation as a marker of low well-being, the city responded with programs that support community engagement. These included weekly group walks, library visits, and art projects, all of which had measurable effects on well-being. More generally, the metrics are critical to establishing the trends and identifying the vulnerable.
In my home state, the Maryland Behavioral Health Administration has programs that teach children growing up with addicted parents how to be resilient, which involves teaching a sense of competency, problem-solving, and coping, among other skills, beginning at the pre-school age through adolescence. Be Well Orange County in California is developing similar programs across the life course.
For
such interventions to be effective over the long-run, they must also help
address the underlying causes of despair, such as lack of employment, sense of
purpose, and hope for the future. These same issues increase
vulnerability to addiction. While reducing isolation and providing
purposeful engagement are effective strategies for older people who are
unlikely to be re-employed, it is important to accompany these with programs to
train the next generation with skills to work in a rapidly changing economy.
These skills can be acquired via vocational or community college education in
some cases. The story
of “comeback” towns in the heartland becoming the hub for the medium
skill jobs outsourced by the tech industry is a promising example.
Communities—or lack there-of—play
an important role in the linkages
between despair, addiction, and premature death. An example of an effort to improve well-being at the
community level comes from the Center for Creative Placehealing at the
University of Louisville, which supports the development of human capacities
for innovation—such as vision, collaboration, and perseverance—and seeks to
intersect these programs with efforts to raise well-being at the community
level. The center’s interventions are based on rigorous
evaluations of pilot efforts.
Expanded federal efforts?
There are, of course, many
related efforts around the country. A federal-level effort to provide collective
evidence and make it available to policymakers and non-governmental
organizations around the country would be an inexpensive first step to jump-start
the process. A bigger step, of course, would be to create a mechanism to provide
federal funds to support such efforts on a systematic basis.
Some 2020 presidential candidates, such as Pete Buttigieg, propose systematic support for efforts that address the root causes, which is heartening, but those plans are in the nascent stages. Other candidates, such as Bernie Sanders, call for solutions focused on the economic problems resulting from trade. Many Republicans highlight the need to tackle immigration and job displacement (read this column by Ross Douthat for more on diverging views regarding causes and possible fixes). The unresolved challenge is that economics, social cohesion, and mental health all intersect in this crisis. No magic bullet will fix it, and the debate is full of false claims and misinformation.
An initial policy, which could generate considerable bang for the buck, is to build well-being metrics into our national statistics collection. For example, the United Kingdom’s government has included four questions in its official statistics for almost a decade that cover life satisfaction, meaning and purpose in life, anxiety, and contentment. These questions are short and inexpensive to administer. Yet they can serve as a national well-being and ill-being tracker. Notable changes among particular cohorts (as we found in our historical data on optimism for less than college educated whites in the 1970s) serve as warning signs of vulnerability. Had we had such signs early on in the U.S., we would not be facing a crisis—and the associated implications for our nation’s health, civic discourse, and politics—of the scale and complexity we have today.
Lessons from minority communities
We
can also learn from the informal safety nets and community support common in
African American and Hispanic communities. These include extended families,
churches, and other social entities that give purpose and meaning to life
beyond an income and a job. Unlike white Americans, who had privileged access
to the good manufacturing and mining jobs, minorities faced historical
discrimination and had to rely on informal safety nets. This experience,
meanwhile, likely led to more empathy for those who fell behind. Ironically, working-class
whites who are now in need are still much less likely to trust the government and
to believe in the importance of education than are minorities. Our work finds
that the gaps in reported well-being across African American and white
communities are the largest among relatively deprived cohorts, such as prime-aged
males out of the labor force.
Sociologist Andrew J. Cherlin of Johns Hopkins University has extensively interviewed children of steelworkers from the now-defunct Bethlehem Steel complex in Baltimore. While African American steelworkers faced significant discrimination, many of their children attended college and moved to better neighborhoods. Yet they return most weeks to the church near the factory and reap the psychological benefit of giving back to their community. The children of the white steelworkers tended not to go to college and remain in the same neighborhood as their parents, but with inferior jobs. While this is not a large sample study, it is surely a very telling one.
My research with Pinto, meanwhile, based on a nationally representative survey, confirms large gaps in faith in the future (and in purpose and meaning) across poor whites and minorities, and shows that they are consistent ones, with the much higher levels of optimism among minorities persisting from well before the 2016 election and lasting afterward. While there is much more to understand, we need to do so if we are going to effectively address our crisis of desperation.
Author

Dig Deeper



The Brookings Institution is committed to quality, independence, and impact.
We are supported by a diverse array of funders. In line with our values and policies, each Brookings publication represents the sole views of its author(s).



Commentary
Understanding the role of despair in America’s opioid crisis
October 15, 2019